FemoroAcetabular Impingement (FAI) is a complex condition that was first described about 15 years ago. Looking back now it is clear that FAI in one form or another has probably been around for hundreds, if not thousands of years.
What is FemoroAcetabular Impingement?
FemoroAcetabular Impingement refers to a condition of the hip where there is abnormal contact (impingement = pinching or conflict) between the ball of the hip (femoral head) and the edge of the socket (acetabulum). This results in local damage to the tissues on the outer margin of the socket – the labrum and the adjacent socket joint surface. These damaged tissues cause hip pain and the abnormal contact between ball and socket generally leads to some restriction of hip movement. The damage created by this abnormal contact situation can become progressively larger and more severe and in theory, in some people if this is unchecked over many years, it may lead to arthritis. It is believed that a number of cases of primary osteoarthritis of the hip where the cause is unknown (idiopathic) could be due to FAI. Whilst a number of these cases of osteoarthritis display features on xray that could be consistent with FAI (anecdotal observation), at present no longitudinal scientific studies (following a group of people over many years and observing what happens to the hip) can prove this link.
What causes FemoroAcetabular Impingement?
FemoroAcetabular Impingement usually results from a mismatch between the ball (femoro) and socket (acetabular) of the hip. In a normal hip the ball is spherical with a convex surface and its shape is matched exactly by the concave surface of the socket. As a result with normal hip movement (flexion/extension, rotation and sideways movement or circumduction) the edge of the ball slides smoothly under the edge of the socket. FAI results when there is a variation/abnormality of the shape of the ball or socket. In this situation certain hip movements result in hard contact, rather than gliding, of the surfaces of the ball and socket – akin to the square peg in a round hole. In general, the greater the shape mismatch, the greater the impingement and the greater the potential for joint damage.
When the shape variation/abnormality is on the ball side of the joint, the condition is known as “cam” type FAI. Generally the ball is aspherical with an elliptical or oval shape. This is the most common type of FAI. When the socket has a shape variation/abnormality, this is referred to as “pincer” impingement. Here the socket is either too deep or the bony edge of the socket is prominent. Sometimes variations/abnormalities of both the socket and ball are present and this is referred to as “mixed” impingement.
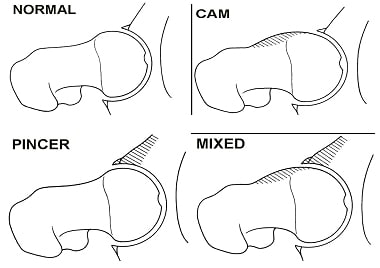
Figure 1. The normal hip (above left) and shape/morphology changes to the ball (femoral head) and socket (acetabulum) leading to different types of femoroacetabular impingement – cam, pincer and mixed.
Abnormalities of the shape of the ball or socket may be congenital (born with this condition) or developmental (develops in childhood or adolescence with bone growth). These abnormalities can be quantified on xray/CT scan/ MRI scan and there are various measures to signify whether the shape differences are mild, moderate or severe. Population studies have identified that at 18 years of age a significant percentage do not have spherical femoral heads (ball). Of these individuals, only a very small number go on to develop the clinical symptoms and signs associated with FAI. This is an important point because FAI is NOT a condition that is diagnosed because an xray or scan report indicates there is a shape variation to the ball or socket.
Occasionally FAI can occur in individuals with normally shaped balls or sockets. These individuals have hypermobile joints and impingement occurs when the joint is at an extreme of its range of movement.

Figure 2. Hypermobility of the hip joint can lead to femoroacetabular impingement in the absence of cam or pincer lesions.
Pathology of FAI
The damage to structures inside the hip joint in FemoroAcetabular Impingement is usually secondary to repeated minor trauma caused by the abnormal contact situation and is therefore “wear and tear” type damage. Occasionally an acute incident can lead to similar damage but this is far less common.
The labrum is a fibro-cartilage structure that attaches to the bony edge of the circumference of the socket. It has a number of different functions – aids in joint stability, helps with synovial fluid distribution, joint surface protection and acts as a joint seal. It has a limited blood supply and therefore has a limited healing capacity. When the labrum is damaged in FAI it is usually due to a shearing type of force which tears the inner surface of this structure where it sits just adjacent to the socket joint surface. The repeated minor trauma to this segment of the labrum in impingement means that this structure has no opportunity to heal itself.
The other structure damaged in FAI is the socket (acetabular) joint surface where it meets the labrum at the edge of the socket. Again it is generally a shearing injury to the joint surface – a layer of gristle like tissue called articular cartilage which is 2 – 3 mm thick and covers and protects the bone of the socket. This causes delamination (stripping a layer) of this surface which can be either partial or full thickness. This creates a flap of tissue (comprised partly of labral tissue and partly articular cartilage) that is unstable and moves abnormally with certain motions of the hip, creating pain and sometimes mechanical symptoms like catching or locking. The articular cartilage layer has no reparative capacity once damaged.
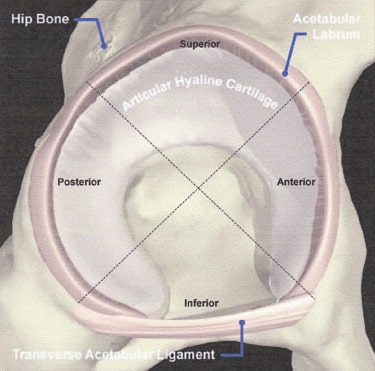
Figure 3. The articular cartilage surface of the socket (acetabulum) of the hip.

Figure 4. An arthroscopic view of damage to the hip labrum and socket joint surface.
Symptoms and Signs of FAI
FemoroAcetabular Impingement is generally symptomatic in younger athletic individuals pursuing sports OR those in the 35-50 year age group who are generally active.
FAI causes pain that is most commonly felt in the groin often during or after sporting activity but can occur whilst sitting or with other activities that require significant hip flexion. Once established, there can be a background groin (much less frequently lateral hip or buttock) ache with sharper exacerbations and sometimes mechanical symptoms like catching or locking. Occasionally individuals will have a feeling of lacking full power in the leg when undertaking activities like cycling. Many people with FAI note reduced flexibility in the hip. Examination of the hip by a specialist will often detect loss of flexion and internal rotation range of motion and reproduction of pain symptoms with certain movements.
Investigations in FAI
Plain xrays (including a good quality lateral view) are really important, as these will often give clues as to issues with the shape of both the femoral head (ball) and acetabulum (socket). Xrays will also detect significant arthritic change.
CT scans (particularly 3D reconstructions) can sometimes be helpful for the doctor in understanding the bone shape mismatches in FAI.

Figure 5. Plain xray of the hip showing bony bump (cam lesion) at the base of the ball.
The definitive investigation however is MRI scan. This complements plain xrays in terms of defining shape variations/abnormalities of the ball and socket but it can also give information about areas of bone stress, accurately reflecting the precise location of abnormal bony contact. MRI is the best current investigation for detecting tears of the labrum and damage/delamination of the adjacent socket joint surface. It is also accurate in determining the extent and severity of any arthritic change within the joint, which is an important factor in guiding treatment.
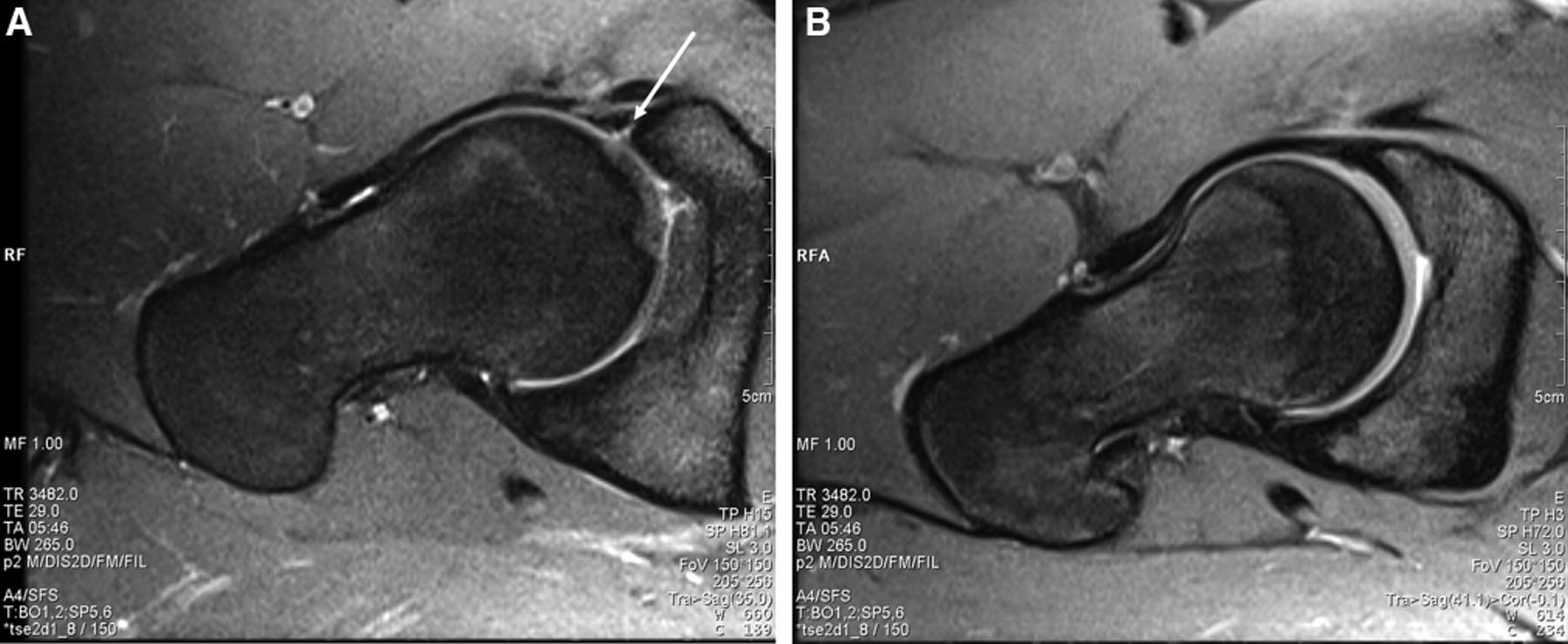
Figure 6. MRI scans. A. Hip with FAI showing cam lesion of ball, labral tear (arrow) and joint surface damage (loss of joint space adjacent to labral tear). B. Normal Hip with spherical ball and normal labrum/joint surface.
Diagnosis of FAI
The diagnosis of FemoroAcetabular Impingement is based on consistency in clinical history, examination findings and radiological investigations. Plain xrays or MRI scan (and reports indicating FAI) alone cannot indicate the presence of FAI – particularly as we now recognize that shape variations/abnormalities are quite common in asymptomatic individuals.
Treatment of FAI
The goals of treatment are to relieve pain, improve function and allow a return to activity.
Non Surgical treatment of FAI
Not every individual with FemoroAcetabular Impongement requires surgery. Many people with FAI can be managed non-operatively. This requires an understanding of the condition and often modification of activities that cause symptoms (mainly pain) – examples include achieving correct bike fit and seating position and pedaling technique for affected cyclists and sometimes simple ergonomic changes to seating at work or in the car.
Analgesic and non steroidal anti-inflammatory medication can be helpful in settling background pain. Sometimes cortisone injections into the hip joint can reduce inflammation and pain but are not indicated in everyone. Once pain has been improved, physiotherapy efforts directed towards avoiding impingement producing movements, strengthening the gluteal and core muscles and stretching fascial tissue can be helpful. As a general rule, individuals with mild symptoms, minimal hip movement restriction and less severe shape abnormalities are good candidates for non-operative treatment.
Surgical treatment of FAI
Surgery for FemoroAcetabular Impingement involves 2 basic principles.
The first of these is to treat the pain causing pathology. This is the damage to the labrum (hip cartilage) and/or the socket joint surface. This involves either trimming or repair of the damaged labrum and trimming, smoothing and sometimes pseudo-repair (called microfracture osteoplasty) of the damaged socket joint surface.
The second principle is to treat shape abnormalities of the ball or socket that have created the damage to the socket margin. This generally means trimming prominent bone from the base of the ball and sometimes from the edge of the socket. This is essential to relieving the abnormal contact/impingement, which is the basis of FAI.
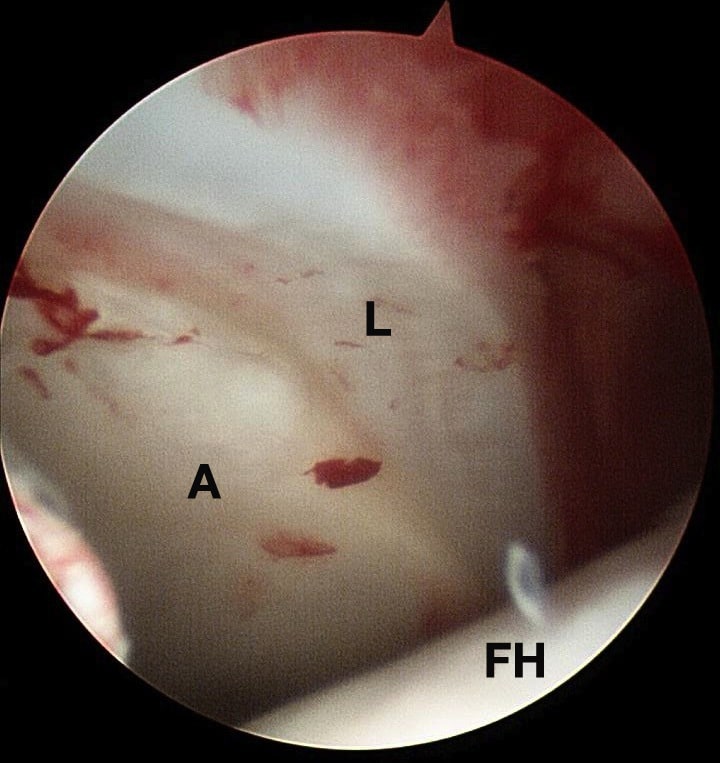
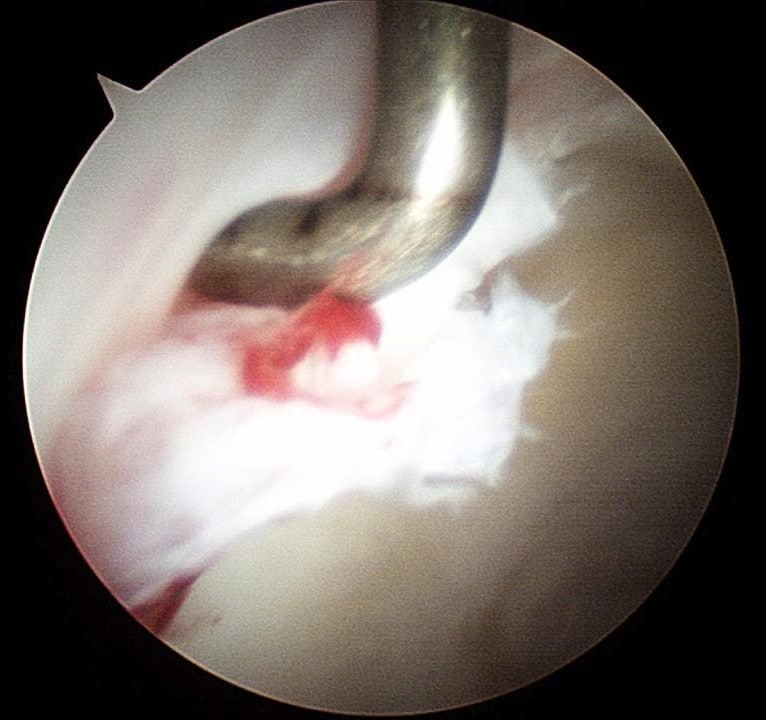

Figure 7. Arthroscopic Treatment of FemoroAcetabular Impingement. LEFT: Normal Labrum (L) and Normal Articular Surface of Socket (A) blend seamlessly together. Femoral Head at bottom (FH). MIDDLE: Typical Socket Rim Lesion with Labral tear and Articular surface damage creating a tissue flap that catches in the joint. RIGHT: Treatment of the Labral/Articular Cartilage flap by debridement and smoothing of the surface defect.
Surgery can be performed arthroscopically (a minimally invasive technique using a small surgical telescope) or by open arthrotomy ( a standard incision with surgical dislocation of the hip to access the joint) or occasionally by a combination of both techniques. The decision regarding surgical technique is based partly on the severity and extent of the problem and partly based on the preference of the surgeon. Most FAI cases requiring surgery can be managed arthroscopically but larger shape abnormalities/more marked areas of joint surface damage are sometimes best managed by open arthrotomy. Both techniques have been demonstrated to be effective in treating FAI.
Unfortunately like with any surgery, surgery for FAI is not universally successful. Outcomes are variable but people with minimal joint surface damage tend to do best. Conversely individuals who have an established arthritis with FAI have poor outcomes following surgery.
Recovery following surgery is often quite prolonged. The first 6 – 8 weeks are spent undertaking light or low impact activity only followed by gradual loading of the hip together with progressive strengthening. Running may be possible after 3 months followed by agility drills and a return to sport at around 5 – 6 months. This timeframe is a general guide but may vary from case to case.
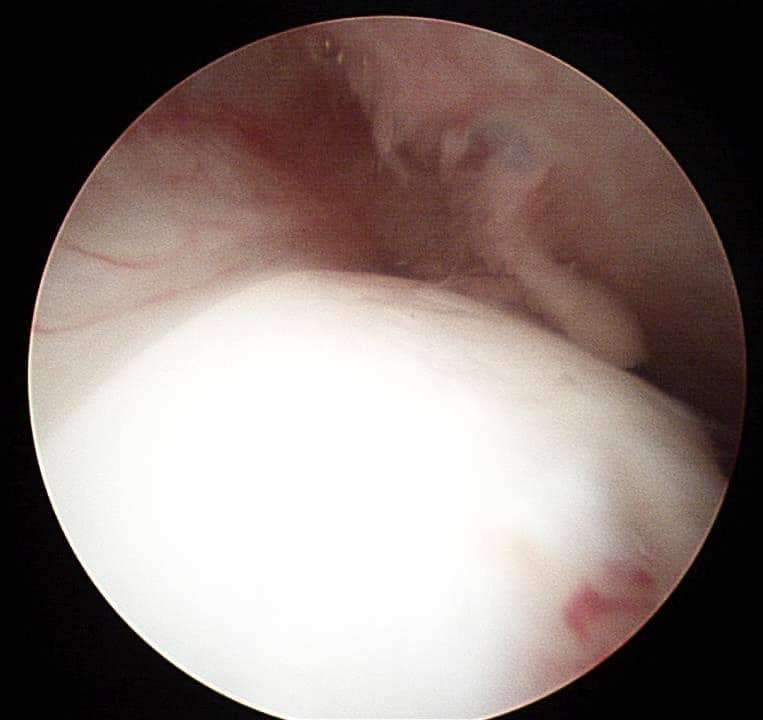
Figure 8. Arthroscopic Treatment of FemoroAcetabular Impingement. LEFT: A typical cam lesion of the femoral (ball) head/neck junction. The labrum is seen in the upper left of the picture. RIGHT: Resection of the cam bone prominence from the femoral head/neck junction – so called femoral osteectomy.
The last word on FemoroAcetabular Impingement
“The impact of surgery on long term clinical results, the natural history of FAI, or the prevention of or delay in the onset of osteoarthritis has not been established. The current literature supports surgical intervention for the treatment of FAI to provide pain relief and improved function in active patients in whom osteoarthritis is not severe, but it does not support prophylactic surgical intervention in asymptomatic individuals to prevent degenerative changes of the hip.” Bedi et al. J Bone Joint Surg Am 2013: 95: 82-92.
Source: https://www.parkclinic.com.au/femoroacetabular-impingement-fai/